
Thyroid Hormone Resistance (RTH), also known as Refetoff Syndrome, is a rare genetic endocrine disorder that fundamentally challenges how we understand hormone function in the human body. Unlike traditional thyroid disorders—where hormone levels directly correlate with symptoms—RTH presents a paradox: elevated thyroid hormones with reduced biological effect.
This condition highlights a crucial concept in modern medicine: hormone levels alone do not define physiological outcomes. Instead, cellular response, receptor sensitivity, and genetic signaling pathways play equally important roles.
First described by Samuel Refetoff in 1969, this syndrome has since become a cornerstone example of hormone resistance disorders, influencing research in endocrinology, genetics, and personalized medicine.
Understanding RTH provides insight not only into thyroid function but also into broader biological mechanisms, including hormone signaling, receptor mutations, and gene expression regulation.
👉 This makes Thyroid Hormone Resistance a unique condition that bridges endocrinology, genetics, and precision medicine.
What Is Thyroid Hormone Resistance?
Thyroid Hormone Resistance (Refetoff Syndrome) is a rare genetic condition, affecting how cells respond to thyroid hormones, primarily:
- T3 (triiodothyronine) – the active hormone
- T4 (thyroxine) – the storage form
In healthy individuals, these hormones regulate:
- Metabolism
- Heart rate
- Brain development
- Body temperature
- Energy production
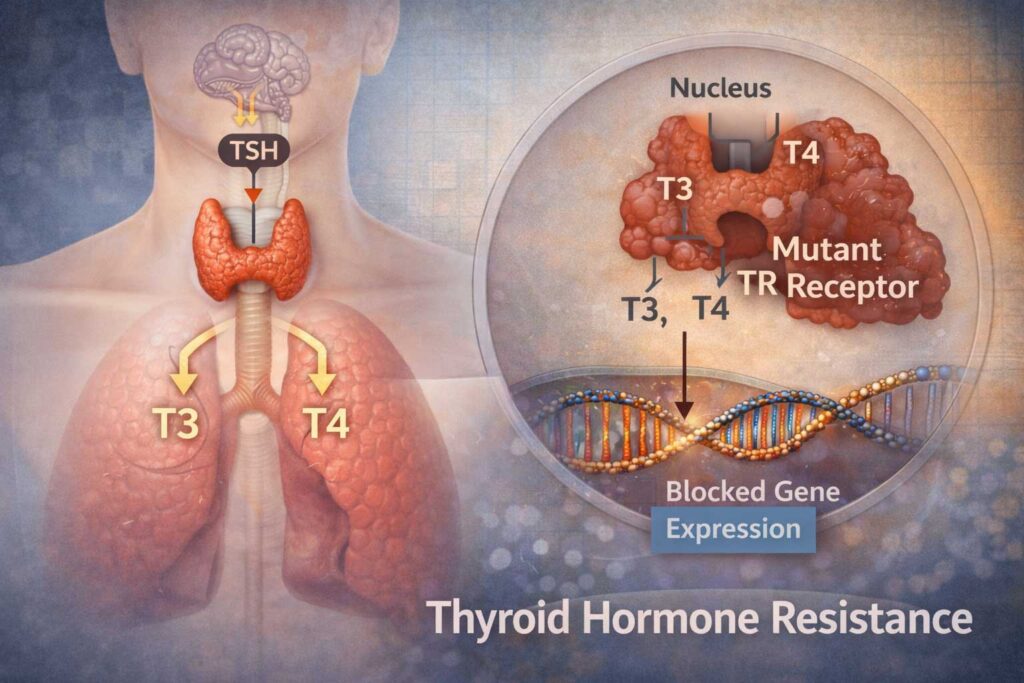
However, in RTH:
- Blood levels of T3 and T4 are elevated
- TSH (thyroid-stimulating hormone) is not suppressed as expected
This creates a paradoxical lab profile that often confuses clinicians.
👉 In simple terms: The body has the hormone—but the cells don’t “listen” to it properly.
Historical Discovery and Bulgarian Connection
The condition was first identified by Samuel Refetoff and colleagues in a landmark 1967–1969 study describing a family with:
- Goiter
- Elevated protein-bound iodine
- Hearing abnormalities
- Skeletal changes
Refetoff proposed that the issue was not hormone production—but target tissue resistance, a groundbreaking idea at the time.
His work laid the foundation for understanding:
- Hormone receptor defects
- Genetic endocrine disorders
- Personalized hormone signaling
He also identified related syndromes, including:
- Resistance to thyrotropin (RTSH)
- Disorders involving the SECISBP2 gene, affecting hormone metabolism
How Thyroid Hormones Normally Work
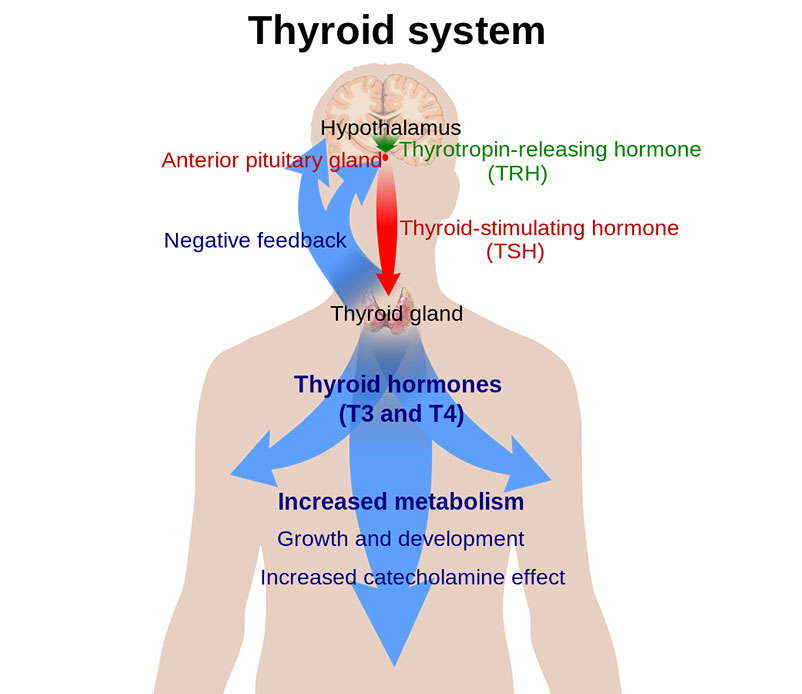
To understand RTH, we must first understand the normal pathway.
Step-by-Step Hormone Action
- Thyroid gland produces T4 and T3
- Hormones enter bloodstream
- They travel into cells
- Bind to nuclear thyroid hormone receptors
- Activate gene expression
This process depends on multiple steps:
- Transport across cell membranes
- Conversion (T4 → T3)
- Binding to receptors
- Gene transcription
If any step fails → resistance occurs.
This process regulates:
- Metabolism
- Growth
- Brain development
- Cardiovascular function
Pathophysiology of Thyroid Hormone Resistance
In Thyroid Hormone Resistance, the problem lies primarily in cellular response, not hormone production.
Key Causes
The most common cause is mutation in:
- THRB gene
This gene encodes the beta thyroid hormone receptor, which is responsible for:
- Binding thyroid hormones
- Activating gene transcription
Other Associated Genes
- SECISBP2 – affects hormone metabolism
- MCT8 – affects hormone transport into cells
The most common cause of Thyroid Hormone Resistance is mutation in the THRB gene, which encodes the beta thyroid hormone receptor. Over 100 different mutations have been identified, affecting receptor function and hormone signaling.
Additional Genetic Factors
- MCT8 → impaired hormone transport
- SECISBP2 → defective hormone metabolism
Molecular Mechanisms and Types of Thyroid Hormone Resistance
Thyroid Hormone Resistance (Refetoff Syndrome) is not a single uniform condition. Instead, it represents a spectrum of disorders caused by disruptions in hormone signaling at the molecular and cellular levels.
👉 These disruptions affect how thyroid hormones interact with receptors and regulate gene expression across different tissues.
Types of Thyroid Hormone Resistance
The clinical presentation of RTH depends on which tissues are affected and to what extent. This leads to two main recognized forms of the condition.
1. Generalized Resistance (GRTH)
Generalized Resistance to Thyroid Hormone (GRTH) is the most common form.
Key Characteristics
- Most or all tissues show reduced sensitivity to thyroid hormones
- The body compensates by producing higher levels of T3 and T4
- Despite elevated hormone levels, many patients appear clinically normal
Clinical Presentation
- Patients are often euthyroid, meaning they show no clear signs of overactive or underactive thyroid function
- Symptoms, if present, tend to be mild
- Goiter may develop due to chronic stimulation of the thyroid gland
👉 This form highlights how the body adapts to resistance by increasing hormone production while maintaining overall balance.
2. Pituitary Resistance (PRTH)
Pituitary Resistance to Thyroid Hormone (PRTH) is less common but clinically significant.
Key Characteristics
- The pituitary gland is less responsive to thyroid hormone feedback
- TSH secretion remains inappropriately normal or elevated
- Other tissues may still respond to thyroid hormones
Clinical Presentation
- Symptoms may resemble hyperthyroidism, including increased heart rate and restlessness
- Patients may experience signs of hormone excess in certain organs
👉 This selective resistance leads to a mismatch between hormone production and feedback regulation.
Symptoms and Clinical Presentation
One of the most distinctive features of Thyroid Hormone Resistance is its highly variable presentation.
Even individuals within the same family—carrying the exact same genetic mutation—can exhibit very different symptoms.
Common Symptoms
The most frequently observed clinical features include:
- Goiter (enlarged thyroid gland)
- Tachycardia (increased heart rate)
- Mild hyperactivity or restlessness
- Learning difficulties or reduced concentration
These symptoms are typically less severe than those seen in classic hyperthyroidism.
Possible Associations
Some studies have identified associations between RTH and:
- Attention-related issues, including patterns similar to ADHD
- Mood disorders, such as depression or emotional instability
👉 Important note: Most individuals with ADHD or depression do NOT have Thyroid Hormone Resistance. These associations are relatively rare and should not be overinterpreted.
Why Symptoms Vary So Much
The variability in symptoms is one of the defining characteristics of RTH and can be explained by differences in how various tissues respond to thyroid hormones.
Key Reasons for Variability
- Different tissues respond differently to thyroid hormones
- Some organs may remain sensitive, while others are resistant
- Variations in genetic mutations affect receptor function differently
- Co-regulators and signaling pathways vary between tissues
Real-World Example
- The heart may remain sensitive to thyroid hormones → leading to tachycardia
- The brain may be more resistant → resulting in normal cognition
Mixed Clinical Picture
This creates a situation where:
- Some systems behave as if thyroid hormone levels are high
- Others behave as if levels are normal
👉 The result is a mixed or inconsistent clinical presentation, which is a hallmark of Thyroid Hormone Resistance.
Why This Matters Clinically
Because symptoms are inconsistent:
- Diagnosis becomes more challenging
- Standard treatment approaches may not apply
- Individualized evaluation is essential
👉 Ultimately, the diversity of symptoms in RTH reflects the complexity of hormone signaling across different tissues—and highlights why this condition remains one of the most intriguing disorders in endocrinology.
Diagnosis of Thyroid Hormone Resistance
Diagnosing Thyroid Hormone Resistance (Refetoff Syndrome) requires careful clinical evaluation because it closely mimics more common thyroid disorders. The condition often presents with confusing laboratory findings that can lead to misinterpretation if not recognized properly.
Unlike typical thyroid diseases, where hormone levels and symptoms align clearly, RTH presents a paradox that requires a deeper understanding of endocrine physiology.
Key Laboratory Findings
The hallmark laboratory pattern of RTH includes:
- Elevated T3 (triiodothyronine)
- Elevated T4 (thyroxine)
- Normal or slightly elevated TSH (thyroid-stimulating hormone)
This combination is highly unusual.
👉 In most cases of elevated thyroid hormones, TSH would be suppressed due to negative feedback.
Why This Pattern Is Confusing
Because of these findings, RTH is often mistaken for:
- Hyperthyroidism, where hormone levels are high and TSH is low
- Pituitary tumors (TSH-secreting adenomas), where TSH remains elevated
Without proper evaluation, patients may receive incorrect diagnoses and unnecessary treatments.
Additional Testing
To confirm Thyroid Hormone Resistance, further investigation is required.
Genetic Testing
The most definitive test involves identifying mutations in the:
- THRB gene
Genetic confirmation helps distinguish RTH from other thyroid disorders.
Family History
Because RTH is often inherited:
- A detailed family history can reveal similar patterns
- Relatives may have mild or undiagnosed forms of the condition
Imaging (When Needed)
Imaging studies may be used to rule out other conditions:
- Pituitary MRI → to exclude TSH-secreting tumors
- Thyroid ultrasound → to evaluate goiter or structural changes
These tests are not used to diagnose RTH directly, but to eliminate alternative causes.
Differential Diagnosis
Accurate diagnosis requires ruling out other conditions that may present similarly.
Doctors must exclude:
- Thyroid hormone overproduction (true hyperthyroidism)
- TSH-secreting pituitary tumors
- Thyroid hormone misuse or medication effects
- Laboratory errors or assay interference
Why Diagnosis Is Challenging
Thyroid Hormone Resistance is considered a diagnostic challenge because:
- It is rare
- Its lab profile is counterintuitive
- Symptoms may be mild or inconsistent
- It overlaps with more common conditions
👉 Awareness and careful interpretation of lab results are essential to avoid misdiagnosis.
Treatment and Management
There is no single standardized treatment for Thyroid Hormone Resistance, as many individuals do not require active intervention.
Management is highly individualized and focuses on symptom control rather than normalizing lab values.
When Treatment Is Needed
Treatment is typically considered when symptoms interfere with daily life.
Common indications include:
- Persistent tachycardia
- Anxiety or restlessness
- Significant goiter
- Cardiovascular symptoms
Symptom-Based Treatment Approach
Beta-Blockers
- Used to control heart rate and reduce palpitations
- Particularly helpful in patients with tachycardia
Monitoring Thyroid Levels
- Regular blood tests to track T3, T4, and TSH
- Helps ensure stability and avoid overtreatment
Avoiding Unnecessary Treatment
- Anti-thyroid medications are usually not appropriate
- Thyroid suppression therapy can be harmful in RTH
Important Clinical Principle
👉 Treat the patient, not just the lab results
Because hormone levels are often elevated in RTH, treating based solely on lab values can lead to incorrect management.
Clinical symptoms and overall well-being should guide treatment decisions.
Long-Term Outlook
Most individuals with Thyroid Hormone Resistance:
- Lead normal, healthy lives
- Require minimal medical intervention
- Benefit from regular monitoring rather than aggressive treatment
Genetic Inheritance
Thyroid Hormone Resistance is most commonly inherited in an autosomal dominant pattern.
What This Means
- Only one mutated gene is required to cause the condition
- A parent with RTH has a 50% chance of passing it to their child
- Both males and females are equally affected
Sporadic Cases
Although most cases are inherited:
- Some individuals develop new (sporadic) mutations
- These occur without a family history
Family Implications
Because of the genetic nature of RTH:
- Family members may benefit from screening
- Genetic counseling can help assess risk
- Early identification can prevent misdiagnosis
Why Genetics Matters
Understanding the genetic basis of RTH:
- Confirms the diagnosis
- Guides clinical management
- Supports personalized medical care
👉 Ultimately, the diagnosis and management of Thyroid Hormone Resistance require a combination of clinical awareness, genetic insight, and careful interpretation of laboratory data.
Hormone Resistance vs Other Disorders
| Condition | Hormone Level | Response |
|---|---|---|
| Hypothyroidism | Low | Low |
| Hyperthyroidism | High | High |
| Thyroid Hormone Resistance (RTH) | High | Reduced |
Advanced Molecular Mechanisms
At a deeper molecular level, Thyroid Hormone Resistance (Refetoff Syndrome) is not simply a receptor defect—it is a complex disruption of multiple interconnected biological systems that regulate how thyroid hormones influence gene expression.
Nuclear Receptor Signaling
Thyroid hormones act through nuclear receptors, especially those encoded by the THRB gene. These receptors regulate gene activity by binding to DNA.
In RTH:
- Mutated receptors have reduced affinity for T3
- Hormone-receptor binding becomes inefficient
- Signal transmission to DNA is impaired
This results in reduced activation of genes responsible for metabolism and energy balance.
DNA Transcription Pathways
Once hormones bind to receptors, they regulate gene expression through transcription.
In RTH:
- Tissue responses vary significantly
- Gene activation is impaired
- Target genes may not respond despite high hormone levels
Co-Activator and Co-Repressor Dysfunction
Proper signaling requires interaction with regulatory proteins.
In RTH:
- Reduced co-activator recruitment weakens signaling
- Co-repressor imbalance disrupts gene regulation
Epigenetic Factors
Histone acetylation plays a role in gene accessibility.
- Abnormal acetylation can suppress hormone-responsive genes
- Leads to reduced cellular response
Hormone Transport Defects
Hormones must enter cells to function.
- Transporter defects (e.g., MCT8) limit intracellular hormone levels
- Circulating hormone may be high, but cellular activity remains low
👉 This makes RTH a model disease for studying hormone resistance, demonstrating that hormone function depends on an entire signaling network—not just hormone levels.
Comparison With Other Hormone Resistance Disorders
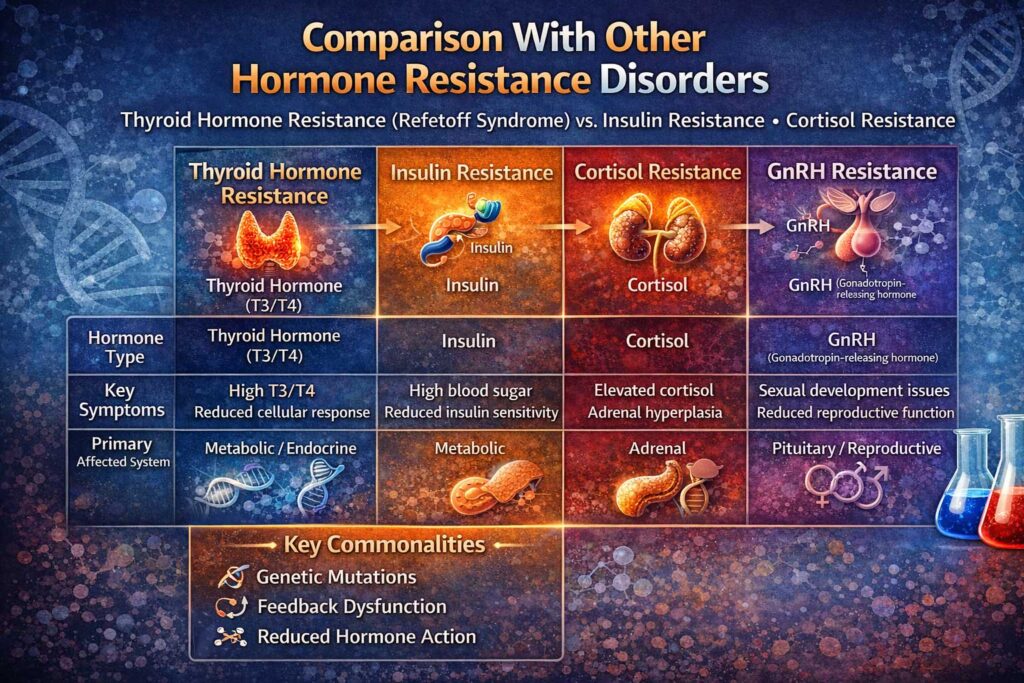
Thyroid Hormone Resistance shares fundamental similarities with several other endocrine disorders.
Related Conditions
RTH is often compared to:
- Insulin resistance – where cells fail to respond properly to insulin
- Vitamin D resistance – affecting calcium balance and bone health
- Androgen resistance – impacting sexual development and hormone signaling
Shared Biological Principle
All of these conditions follow the same core concept:
👉 The hormone is present, but the body’s response is impaired
This highlights a key paradigm in endocrinology:
- Hormone concentration alone is not enough
- Cellular sensitivity determines the actual biological effect
Thyroid Hormone Transport and Metabolism
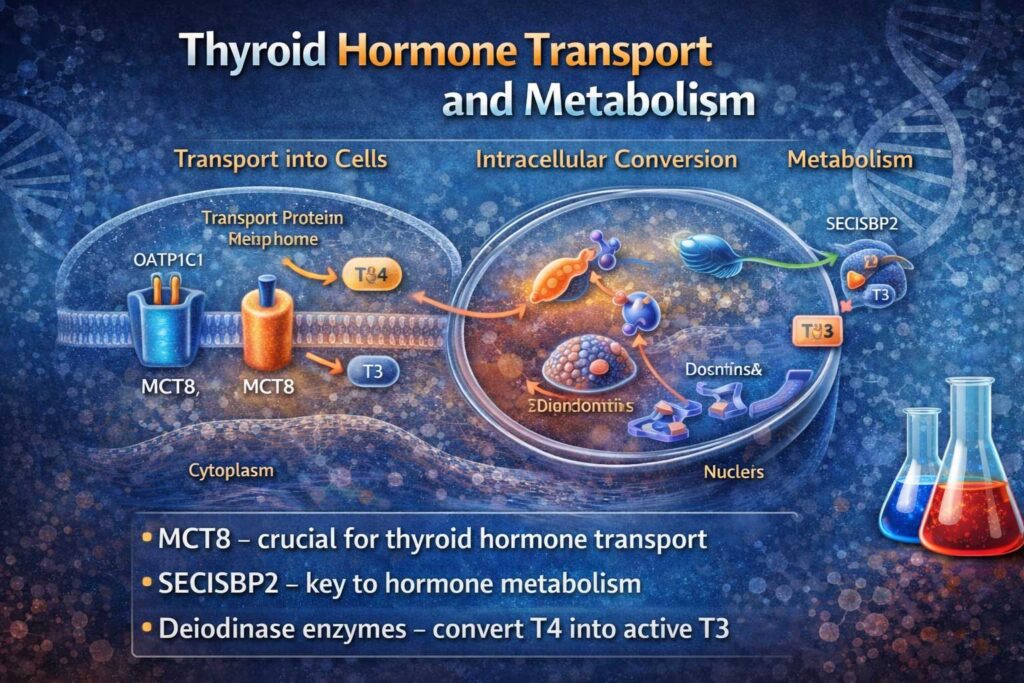
Normal thyroid function depends on multiple steps:
Membrane Transporters
- Allow hormones to enter cells
- Defects reduce intracellular availability
Deiodinase Enzymes
- Convert T4 into active T3
- Impairment reduces hormone activity
Nuclear Receptors
- Control gene expression
- Mutations (THRB) disrupt signaling
👉 Failure at any step can lead to thyroid hormone resistance.
Integrated System Failure
If any step in this pathway fails:
- Transport
- Conversion
- Receptor binding
👉 The result can be partial or complete thyroid hormone resistance.
RTH and Neurodevelopment
Thyroid hormones play a critical role in brain development and neurological function, especially during early life.
Potential Neurological Effects
Some studies suggest that RTH may be associated with:
- Cognitive differences
- Behavioral changes
- Attention regulation issues
In particular, there has been research exploring links between RTH and attention-related conditions.
Important Clarification
While associations have been observed:
- Most individuals with ADHD or behavioral disorders do not have RTH
- The relationship is complex and not fully understood
Current Scientific Perspective
Research in this area is ongoing, and conclusions remain limited.
Scientists continue to investigate:
- How thyroid hormones influence brain signaling
- The role of receptor mutations in neurodevelopment
- Long-term cognitive outcomes in individuals with RTH
Why This Matters
Understanding the neurological impact of thyroid hormone resistance may:
- Improve early diagnosis
- Guide treatment strategies
- Provide insight into broader brain-hormone interactions
👉 Overall, RTH offers a unique window into how hormones influence not just metabolism—but also brain function and development.
Research and Future Directions
Modern research into Thyroid Hormone Resistance (Refetoff Syndrome) is advancing rapidly, driven by breakthroughs in genetics, molecular biology, and precision medicine. Because RTH is rooted in receptor dysfunction and cellular signaling abnormalities, it has become an important model for studying how hormones interact with genes and tissues.
Gene Therapy
One of the most promising areas of research is gene therapy, which aims to correct the underlying genetic mutations responsible for the condition—most commonly those affecting the THRB gene.
Scientists are exploring techniques such as:
- Targeted gene editing (e.g., CRISPR-based approaches)
- Gene replacement strategies
- RNA-based therapies to improve receptor expression
While still largely experimental, gene therapy holds the potential to address the root cause of thyroid hormone resistance rather than just managing symptoms.
👉 This positions Thyroid Hormone Resistance as a key model for the future of precision medicine and targeted endocrine therapies.
Targeted Receptor Modulation
Another key research direction involves developing therapies that can enhance or bypass defective thyroid hormone receptors.
This includes:
- Selective thyroid hormone analogs that bind more effectively to mutated receptors
- Molecules designed to improve receptor sensitivity
- Drugs that modify co-activator and co-repressor interactions
These approaches aim to restore normal signaling at the cellular level, even in the presence of genetic mutations.
Personalized Endocrinology
RTH has become a leading example of personalized endocrinology, where treatment is tailored to an individual’s unique genetic and biochemical profile.
Future clinical approaches may include:
- Genetic profiling to identify specific mutations
- Customized hormone therapies based on receptor function
- Individualized monitoring strategies rather than standard reference ranges
This shift reflects a broader trend in medicine toward precision treatment, where therapies are designed for the individual rather than the average patient.
Expanding Scientific Understanding
Beyond treatment, RTH continues to provide valuable insights into fundamental biological processes.
Researchers use this condition to better understand:
- Hormone signaling pathways and how they regulate metabolism
- Gene expression mechanisms, including nuclear receptor activity
- The role of transport proteins and enzymes in hormone activation
These discoveries extend far beyond thyroid disease and contribute to the understanding of many other endocrine and metabolic conditions.
Why Refetoff Syndrome Matters
Thyroid Hormone Resistance is more than a rare disorder—it represents a major turning point in medical science.
A Paradigm Shift in Endocrinology
Before its discovery, endocrine disorders were primarily understood in terms of hormone levels alone. Refetoff Syndrome challenged this view by demonstrating that:
👉 Hormone levels alone do not define disease
Instead, the body’s response at the cellular level is equally important.
Introduction of New Concepts
The study of RTH introduced several foundational concepts that are now central to modern medicine:
- Tissue-level hormone sensitivity – different organs can respond differently to the same hormone levels
- Receptor-based disorders – diseases caused by defects in hormone receptors rather than hormone production
- Signal transduction defects – disruptions in how signals are transmitted within cells
These ideas have reshaped how clinicians approach not only thyroid disorders but also a wide range of hormonal conditions.
Broader Medical Impact
The principles uncovered through RTH research apply to many other diseases, including:
- Insulin resistance in diabetes
- Hormone-resistant cancers
- Genetic metabolic disorders
By understanding how and why the body becomes resistant to hormonal signals, researchers can develop more effective and targeted treatments across multiple fields of medicine.
A Model for the Future of Medicine
Refetoff Syndrome continues to serve as a model for:
- Precision medicine
- Genetic diagnostics
- Targeted therapies
It highlights the importance of integrating genetics, molecular biology, and clinical practice to achieve better patient outcomes.
👉 Ultimately, Thyroid Hormone Resistance teaches one of the most important lessons in medicine:
It is not just the presence of a hormone that matters—but how the body responds to it.
Misdiagnosis and Clinical Challenges
Thyroid Hormone Resistance (Refetoff Syndrome) is one of the most commonly misinterpreted endocrine conditions due to its unusual laboratory profile. The combination of elevated thyroid hormones (T3 and T4) with a non-suppressed thyroid-stimulating hormone (TSH) often leads clinicians toward more common diagnoses.
Conditions RTH Is Often Mistaken For
Because of overlapping symptoms and lab findings, RTH may be misdiagnosed as:
- Graves’ disease – due to elevated thyroid hormone levels and symptoms like tachycardia
- Anxiety disorders – especially when patients present with restlessness, palpitations, or nervousness
- Pituitary tumors (TSH-secreting adenomas) – because TSH is not suppressed as expected
In some cases, patients may undergo extensive testing or even inappropriate treatments before the correct diagnosis is made.
Consequences of Misdiagnosis
Misdiagnosis can lead to:
- Unnecessary treatments, including anti-thyroid medications
- Incorrect hormone suppression therapies
- Unwarranted imaging or invasive procedures
- Psychological stress from unclear or conflicting diagnoses
This highlights the importance of recognizing the unique biochemical pattern of RTH and considering genetic testing when appropriate.
👉 Accurate diagnosis is critical to avoid overtreatment and ensure proper management.
Broader Impact on Endocrinology
Thyroid Hormone Resistance is not just a rare condition—it serves as a powerful model for understanding a wide range of hormonal disorders.
A Model for Hormone Resistance
RTH has helped shape the understanding of other conditions where hormones are present but not fully effective, including:
- Insulin resistance – seen in type 2 diabetes
- Vitamin D resistance – affecting bone metabolism
- Androgen resistance – impacting sexual development
- Other hormone signaling disorders involving receptor or pathway dysfunction
Why It Matters
These conditions share a common principle:
👉 The presence of a hormone does not guarantee a biological response
By studying RTH, researchers have gained deeper insights into how hormones interact with receptors, genes, and cellular machinery—knowledge that extends far beyond thyroid disease.
Clinical Case Study: A Real-World Example of Thyroid Hormone Resistance
To better understand how Thyroid Hormone Resistance (Refetoff Syndrome) presents in clinical practice, consider the following representative case scenario.
Patient Presentation
A 28-year-old patient presents with:
- Persistent elevated heart rate (tachycardia)
- Occasional anxiety and restlessness
- Mild enlargement of the thyroid gland (goiter)
Despite these symptoms, the patient reports:
- Normal energy levels
- Stable weight
- No heat intolerance or excessive sweating
This mixed clinical picture raises initial suspicion of a thyroid disorder, but does not fully align with classic hyperthyroidism.
Laboratory Findings
Blood tests reveal:
- Elevated T3 and T4 levels
- TSH within normal range (not suppressed)
This is a key red flag.
👉 In typical hyperthyroidism, TSH would be very low or undetectable.
Initial Misdiagnosis
The patient is initially suspected to have:
- Subclinical hyperthyroidism
- Early Graves’ disease
However, further testing shows:
- No thyroid-stimulating antibodies
- Normal radioactive iodine uptake
At this stage, the diagnosis becomes unclear.
Further Investigation
Due to the unusual lab pattern, an endocrinologist considers Thyroid Hormone Resistance.
Additional steps include:
- Detailed family history
- Genetic testing
- Evaluation of similar symptoms in relatives
Genetic analysis confirms a mutation in the:
- THRB gene
Final Diagnosis
The patient is diagnosed with:
👉 Generalized Thyroid Hormone Resistance (RTH)
Management Approach
Because the patient is largely asymptomatic aside from mild tachycardia:
- No aggressive treatment is initiated
- A low-dose beta-blocker is prescribed for heart rate control
- Regular monitoring is recommended
Outcome
Over time:
- Symptoms remain stable
- No progression of disease
- Patient maintains normal quality of life
Key Clinical Insights
This case highlights several important lessons:
- Elevated thyroid hormones do not always indicate hyperthyroidism
- Normal TSH in the presence of high T3/T4 should raise suspicion for RTH
- Misdiagnosis can lead to unnecessary treatment
- Genetic testing plays a crucial role in confirmation
Why Case Studies Matter
Clinical case studies like this help bridge the gap between theory and real-world practice. They illustrate how complex conditions such as Thyroid Hormone Resistance can present subtly and require careful evaluation.
👉 For clinicians, recognizing these patterns is essential
👉 For patients, it emphasizes the importance of accurate diagnosis and second opinions when needed
Comparison: Thyroid Hormone Resistance vs Graves’ Disease vs Hyperthyroidism
Understanding the differences between Thyroid Hormone Resistance (Refetoff Syndrome) and more common thyroid disorders such as Graves’ disease and hyperthyroidism is critical for accurate diagnosis and proper treatment.
Although these conditions may appear similar at first—especially in lab results—they differ significantly in their underlying mechanisms and clinical presentation.
Key Differences at a Glance
| Feature | Thyroid Hormone Resistance (RTH) | Graves’ Disease | Hyperthyroidism (General) |
|---|---|---|---|
| Cause | Genetic mutation (often THRB gene) | Autoimmune (antibodies stimulate thyroid) | Various (nodules, inflammation, excess hormone) |
| T3 / T4 Levels | High | High | High |
| TSH Levels | Normal or slightly elevated | Suppressed (very low) | Suppressed |
| Hormone Response | Reduced (tissue resistance) | Increased (overactive thyroid) | Increased |
| Goiter | Common | Common | Sometimes |
| Heart Rate | Mild to moderate increase | Often significantly elevated | Elevated |
| Eye Symptoms (Exophthalmos) | Rare | Common | Rare |
| Metabolism | Mixed / near normal | Increased | Increased |
| Weight Changes | Often stable | Weight loss common | Weight loss common |
| Diagnosis Challenge | High (often misdiagnosed) | Moderate | Low |
| Genetic Component | Yes (autosomal dominant) | No (autoimmune) | Usually no |
| Treatment Approach | Often observation, symptom control | Anti-thyroid drugs, radioactive iodine | Depends on cause |
Why This Comparison Matters
Thyroid Hormone Resistance is frequently confused with hyperthyroidism because both conditions show elevated thyroid hormone levels. However, the key difference lies in how the body responds:
- In Graves’ disease and hyperthyroidism, the body is overstimulated by thyroid hormones
- In RTH, the body is partially resistant, leading to a mixed or normal metabolic state
👉 This distinction is critical because treating RTH as hyperthyroidism can lead to unnecessary and potentially harmful treatments.
Diagnostic Clue to Remember
The most important differentiating factor:
👉 TSH behavior
- Suppressed TSH → likely hyperthyroidism or Graves’ disease
- Normal or elevated TSH → consider Thyroid Hormone Resistance
Clinical Insight
A patient with:
- High T3/T4
- Normal TSH
- Mild or inconsistent symptoms
Should always raise suspicion for RTH rather than classic hyperthyroidism.
Lifestyle and Supportive Care
Although Thyroid Hormone Resistance (Refetoff Syndrome) is a genetic condition and cannot be reversed through lifestyle changes alone, adopting healthy daily habits can significantly improve overall well-being and help manage symptoms more effectively.
Supportive care focuses on optimizing the body’s ability to function despite reduced sensitivity to thyroid hormones. This includes maintaining balance across metabolic, cardiovascular, and mental health systems.
Balanced Nutrition
A well-balanced diet plays an important role in supporting thyroid health and overall endocrine function. While nutrition does not directly correct hormone resistance, it helps regulate energy levels, stabilize metabolism, and reduce additional stress on the body.
Key nutritional principles include:
- Consuming whole, unprocessed foods
- Including healthy fats, lean proteins, and complex carbohydrates
- Ensuring adequate intake of micronutrients such as selenium, zinc, and iodine
- Supporting gut health, which plays a role in hormone metabolism
A nutrient-rich diet helps maintain stable energy and may reduce symptoms such as fatigue, mood fluctuations, and metabolic imbalance.
Stress Management
Chronic stress can negatively impact hormonal balance and worsen symptoms associated with thyroid disorders. The body’s stress response—regulated by cortisol—can interfere with endocrine function and amplify issues like rapid heart rate, anxiety, and fatigue.
Effective stress management strategies include:
- Mindfulness practices such as meditation or deep breathing
- Regular physical activity
- Spending time outdoors
- Maintaining a consistent daily routine
Reducing stress supports the body’s regulatory systems and can improve overall symptom control.
Regular Monitoring
Ongoing medical monitoring is essential for individuals with thyroid hormone resistance. Because the condition can present with fluctuating symptoms and unusual lab results, regular follow-up with a healthcare provider ensures appropriate management.
Monitoring typically includes:
- Periodic blood tests (T3, T4, TSH levels)
- Clinical evaluation of symptoms
- Cardiovascular monitoring if tachycardia is present
- Genetic counseling when applicable
Close monitoring helps prevent unnecessary treatments and ensures that any changes in the condition are addressed early.
Holistic Approach to Living with RTH
Living with Thyroid Hormone Resistance requires a holistic approach that combines medical guidance with lifestyle optimization. While the condition itself is rare and complex, many individuals lead normal, active lives by maintaining healthy habits and staying informed about their condition.
👉 The goal is not to “fix” the hormone levels, but to support the body’s ability to function optimally despite reduced hormone sensitivity.
FAQs About Thyroid Hormone Resistance (Refetoff Syndrome)
What is Refetoff Syndrome?
Refetoff Syndrome, also known as Thyroid Hormone Resistance (RTH), is a rare genetic disorder in which the body’s tissues do not respond properly to thyroid hormones despite normal or elevated hormone levels in the blood.
Is it dangerous?
In most cases, Refetoff Syndrome is not dangerous. Many individuals live normal, healthy lives with minimal or no symptoms, especially when the condition is properly monitored.
Can it be cured?
There is currently no cure for thyroid hormone resistance. However, symptoms can be effectively managed through monitoring and, in some cases, targeted treatments.
Is it inherited?
Yes, thyroid hormone resistance is most commonly inherited in an autosomal dominant pattern, meaning a single copy of the mutated gene can cause the condition.
How rare is it?
Refetoff Syndrome is considered extremely rare, affecting a very small number of individuals worldwide. Some cases may remain undiagnosed due to its mild or variable symptoms.
Can thyroid hormone resistance be mistaken for hyperthyroidism?
Yes, it is often mistaken for hyperthyroidism because patients have elevated thyroid hormone levels, even though their body does not respond to those hormones normally.
Does diet affect thyroid hormone resistance?
Diet cannot cure thyroid hormone resistance, but maintaining a balanced and nutrient-rich diet can support overall thyroid health and improve general well-being.
Can children have Refetoff Syndrome?
Yes, the condition is often diagnosed in childhood, especially in families where the genetic mutation is inherited.
Is surgery required?
No, surgery is rarely required for thyroid hormone resistance, as the condition is typically managed without invasive procedures.
Can lifestyle improve symptoms?
Yes, healthy lifestyle habits such as stress management, quality sleep, and balanced nutrition can help reduce symptoms and support overall endocrine health.
Conclusion
Thyroid Hormone Resistance (Refetoff Syndrome) is a fascinating and complex disorder that challenges traditional medical understanding.
Discovered by Samuel Refetoff, it demonstrates that:
👉 Hormone levels alone do not determine biological function
Instead, the body’s response at the cellular level defines health outcomes.
References
- Refetoff S, DeWind LT, DeGroot LJ (1967). “Familial syndrome combining deaf-mutism, stuppled epiphyses, goiter and abnormally high PBI: possible target organ refractoriness to thyroid hormone.” J. Clin. Endocrinol. Metab. 27 (2): 279–94. https://doi.org/10.1210/jcem-27-2-279
- Weiss RE, Dumitrescu A, Refetoff S (2010). “Approach to the patient with resistance to thyroid hormone and pregnancy.” J. Clin. Endocrinol. Metab. 95 (7): 3094–102. https://doi.org/10.1210/jc.2010-0409
- Refetoff S, Bassett JH, Beck-Peccoz P, Bernal J, Brent G, Chatterjee K, et al. (March 2014). “Classification and proposed nomenclature for inherited defects of thyroid hormone action, cell transport, and metabolism.” Eur Thyroid J. 3 (1): 7–9. https://doi.org/10.1159/000358180
- Hauser P, Zametkin AJ, Martinez P, et al. (1993). “Attention deficit-hyperactivity disorder in people with generalized resistance to thyroid hormone.” N. Engl. J. Med. 328 (14): 997–1001. https://doi.org/10.1056/NEJM199304083281403
- Fardella CE, Artigas RA, Gloger S, Jiménez M, Carvajal CA, Krall PM, Quiroz D, Campino C, Mosso LM (June 2007). “Refractory depression in a patient with peripheral resistance to thyroid hormone (RTH) and the effect of triiodothyronine treatment.” Endocrine. 31 (3): 272–8. https://doi.org/10.1007/s12020-007-0042-7
- Beato-Víbora P, Arroyo-Díez J, Rodríguez-López R (March 2013). “Thyroid hormone resistance caused by a novel deleterious variant of the thyroid hormone receptor beta gene.” Eur. J. Obstet. Gynecol. Reprod. Biol. 167 (1): 118–9. https://doi.org/10.1016/j.ejogrb.2012.11.001
- Refetoff S, Dumitrescu AM (2007). “Syndromes of reduced sensitivity to thyroid hormone: genetic defects in hormone receptors, cell transporters and deiodination.” Best Pract. Res. Clin. Endocrinol. Metab. 21 (2): 277–305. https://doi.org/10.1016/j.beem.2007.03.005
- Bottcher Y, Paufler T, Stehr T, Bertschat FL, Paschke R, Koch CA (2007). “Thyroid hormone resistance without mutations in thyroid hormone receptor beta.” Med. Sci. Monit. 13 (6): CS67–70. https://doi.org/10.12659/MSM.484143
- Lafranchi SH, Snyder DB, Sesser DE, Skeels MR, Singh N, Brent GA, Nelson JC (September 2003). “Follow-up of newborns with elevated screening T4 concentrations.” J. Pediatr. 143 (3): 296–301. https://doi.org/10.1067/S0022-3476(03)00184-7